Apr 4, 2023 | SPORTS BETTING
Read the original article by KAALTV HERE.
By Jessie Klinger
The Minnesota Alliance on Problem Gambling is raising awareness about gambling addiction, as it predicts nearly $10 billion in both legal and illegal bets to be placed during this year’s NCAA Men’s Basketball March Madness.
According to a new survey by the American Gaming Association, 68 million American adults plan to bet on the tournament, meanwhile, 4 – 6 million of which are considered to have mild or moderate gambling problems.
Warning signs of problem gambling include betting more than you can afford to lose, bragging about your wins but never the losses, lying about the amount you’re betting, and spending long periods of time gambling or betting more frequently.
With a majority of people making brackets and bets online, it’s easier to develop these harmful habits.
“The electronic accessibility makes it easier, it also makes it easier for someone to isolate. You can now sit in your home on your phone and nobody knows,” says MNAPG Executive Director Susan Sheridan Tucker. “It’s not that we’re against gambling, we just want it to be safe for all players.”
Some precautions to take when it comes to gambling include setting a time limit, setting a spending limit, checking in with how you feel, and being honest with yourself.
Problem Gambling Awareness Month is also about raising awareness about for resources available to those who do need help with problem gambling.
“There’s a variety of ways that people can approach recovery. For some, it means total abstinence, that’s the way in which it’s going to be helpful for them. For others, it may be just adjusting, that they pull back, take a break,” says Tucker.
Mar 29, 2023 | RESEARCH
Read the original article on The Basis HERE.
Editor’s Note: Today’s review is part of our month-long Special Series on Pathways to Addiction. Throughout March, The BASIS is highlighting risk factors for and pathways to addiction.
The development of the pathways model of problem and pathological gambling in 2002 was an important step towards recognizing the heterogeneity of individuals who face gambling-related harms. The model identified distinct subgroups of people experiencing problem or pathological gambling based on a variety of social, biological, and environmental risk factors. The authors, Alex Blaszczynski and Lia Nower, identified three distinct subtypes of individuals experiencing gambling problems: (1) those who were behaviorally conditioned, (2) those with pre-existing emotional vulnerabilities (e.g., anxiety, depression), and (3) those who reported frequent impulsive and/or antisocial behavior. This week, as a part of our Special Series on Pathways to Addiction, The WAGER reviews a study by Lia Nower and colleagues that updated and revised the original pathways model.
What were the research questions?
Does the pathways model of problem and pathological gambling require revision? What revisions or additions should be made to the pathways model?
What did the researchers do?
The researchers surveyed 1,168 individuals with moderate to severe gambling problems seeking treatment across the United States, Canada, and Australia. Participants completed the Problem Gambling Severity Index (PGSI) and the Gambling Pathways Questionnaire (GPQ). The PGSI is a well-regarded and frequently used research instrument to measure the presence and severity of an individual’s gambling problems. On the other hand, the GPQ is an instrument designed to categorize individuals experiencing problem gambling based on the risk factors that they might have experienced. Using participants’ scores on the 11 subscales of the GPQ, the researchers performed latent class analysis to identify subgroups of individuals experiencing problem gambling.
What did they find?
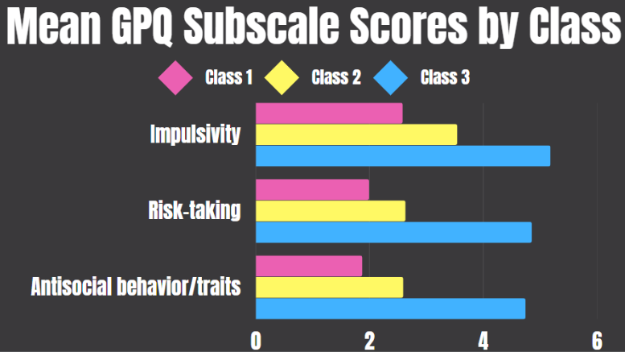
Similar to the original pathways study, the latent class analysis identified three distinct subgroups. Class 1, the largest class, had the lowest average (i.e., mean) scores on each of the GPQ subscales. Class 2 was characterized by high levels of anxiety and depression, both pre- and post-problem gambling, in addition to a high rate of childhood maltreatment (see Figure 1). Finally, Class 3 comprised individuals who scored high in impulsivity and reported frequent risk-taking and/or antisocial behavior (see Figure 2). In terms of problem gambling severity, Class 2 had the highest average scores, while Class 3 scored only slightly lower. Notably, the research team also found some overlap between classes. For example, Classes 2 and 3 both reported gambling to cope with stress, though only Class 3 reported gambling to find meaning.
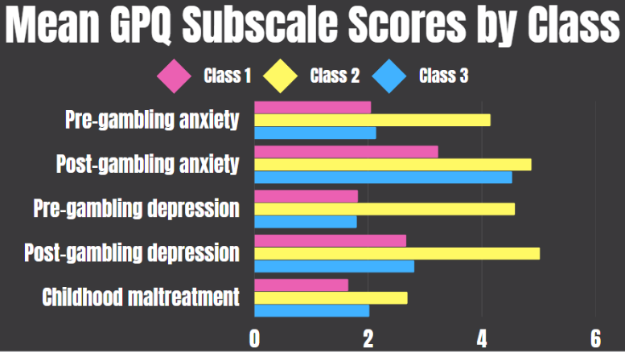
Figure 1. Gambling Pathways Questionnaire (GPQ) subscales that differentiate Class 2 from Classes 1 and 3. The total possible range for each GPQ subscale varies and is calculated by summing the responses within each subscale.
Figure 2. Gambling Pathways Questionnaire (GPQ) subscales that differentiate Class 3 from Classes 1 and 2. The total possible range for each GPQ subscale varies and is calculated by summing the responses within each subscale.
Why do these findings matter?
Recognizing the heterogeneity of pathways to problem gambling within this population is important because it allows treatment professionals to focus on the most salient risk factors for gambling problems rather than more tangential issues. For example, impulsivity is considered an important risk factor for Gambling Disorder and some interventions focus on modulating impulsivity. However, because only a subset of participants experienced heightened impulsivity, it is possible that significantly more people who experience gambling problems would instead benefit from safer product design that disrupts the conditioning aspects of gambling, such as mandatory breaks or the use of self-limit features (e.g., limiting time or amount wagered per gambling session).
Every study has limitations. What are the limitations in this study?
This study only included individuals who were seeking treatment for Gambling Disorder, so the findings might not apply to non-treatment seeking individuals experiencing gambling problems. Additionally, the GPQ measures pre-gambling anxiety/depression by asking participants to retrospectively recall their feelings though research suggests these measures are unreliable.
Mar 29, 2023 | SPORTS BETTING
Legislation needs to include increases in treatment, prevention and research funding to match the proposed expansion of gambling rights.
By Susan Sheridan Tucker
Opinion editor’s note: Star Tribune Opinion publishes a mix of national and local commentaries online and in print each day. To contribute, click here.
•••
March Madness is well underway, and with it a deluge of gambling that propels the tournament. It’s estimated that 1 in 5 Americans will place bets on this year’s NCAA basketball tournament, which creates a hazardous environment for anyone susceptible to problem gambling.
Though most Americans can gamble for enjoyment without issue, the issue of gambling addiction is one that’s gone woefully unaddressed by state and federal addiction programs. It is a fact that gambling addiction produces the highest rate of suicide among addictions, making it a very real public health issue.
As Minnesota lawmakers consider passing a bill that would legalize sports betting, it’s more imperative than ever that the legislation includes increases in treatment, prevention and research funding to match the proposed expansion of gambling rights. It is the mission of the Minnesota Alliance on Problem Gambling (MNAPG) to raise awareness of gambling addiction and advocate for more safeguards around gambling to ensure consumers are protected and able to access resources for treatment and prevention.
It’s no coincidence that March is Problem Gambling Awareness Month. All over the country, organizations like ours make special efforts throughout the month to get the word out that problem gambling is a legitimate addiction defined in the latest edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
Though MNAPG remains neutral on legalization, we stand for the prioritization of consumer protection over revenue. We’ve worked alongside several lawmakers involved in crafting the proposed legislation, which includes a lot of promising language around the following:
Funding: Directing 40% of sports betting tax revenue toward problem gambling programs.
Age restrictions: The promise to raise the legal betting age to 21 will help to prevent high school students from accessing regulated gambling sites on their phones.
Education: Prevention messaging to students, and especially young athletes, will provide a foundational understanding of the harms that can occur with gambling and where one can turn for help. Gambling prevention education is still absent from middle school and high school curricula.
Meanwhile, there are key pieces missing from the current legislation that would be critical to include. They include:
Rule making: MNAPG would prefer to see more specific language built into the bill and will actively participate in the rule-making process to include specific practices requiring operators to build responsible gaming programs. These programs should include comprehensive employee training, access to self-exclusion programs, ability to set limits on time and money spent on betting, and specific requirements for the inclusion of help/prevention messages in external marketing.
Research: There are currently no federal dollars to fund gambling disorder research. Each state must decide whether to support such efforts. MNAPG believes there should be funding for regularly scheduled studies to monitor the impacts of gambling on players and support for using the data to develop evidence-based mitigation efforts. We don’t seek individual data, but would make aggregate data on players’ behaviors and experiences available to universities and nonprofit research entities. Without access to such data, the hands of those who work in the prevention and treatment fields are tied.
No one chooses to become addicted to anything — it’s never due to a moral failing or a lack of willpower. Gambling addiction is just as serious as an alcohol or drug addiction and deserves to be treated equitably, with an appropriate level of funding for treatment, prevention, research and training.
Susan Sheridan Tucker is the executive director of the Minnesota Alliance on Problem Gambling.
Feb 26, 2023 | YOUTH GAMBLING
Read the original article on The Basis HERE.
By Kira Landauer, MPH
Gaming disorder (GD) is characterized by impaired control over playing video games and a continuation or escalation of gaming despite negative consequences. Screening, brief intervention, and referral to treatment (SBIRT) is a popular approach for quickly identifying and addressing substance use disorders, and it may also be beneficial for gaming problems. This week, The WAGER reviews a study by Jennifer J. Park and colleagues that examined clinician attitudes toward and approaches to screening, treatment, and referral for GD in addiction and youth service settings.
What were the research questions?
What are clinician attitudes toward screening for GD in addiction and youth service settings? Which behavioral change techniques would clinicians use to treat GD, and how confident are clinicians in using each technique?
What did the researchers do?
The researchers surveyed 88 experienced clinicians (e.g., counselors, psychologists, social workers) who provide SBIRT to adolescents or adults from 35 gambling, substance use disorder, and youth service programs across New Zealand. They reported their average monthly caseload of clients with GD and completed questionnaires that assessed their attitudes toward screening for GD and the actions they would take if GD was detected in a client. Participants also reported the types of behavioral change techniques1 they would use to treat GD and their level of confidence with each technique. The researchers calculated frequencies, averages, and percentages for the survey items.
What did they find?
Most clinicians had at least one consultation in the past year with someone with gaming-related problems (84.1%) and reported a mean monthly caseload of 4.1 individuals experiencing gaming problems. The majority of clinicians felt somewhat comfortable or very comfortable with screening for GD. Barriers to screening included lack of clinician awareness of available screening tools and the perception that people accessing services would not want to be screened for GD (see Figure). Nearly one-fifth of participants felt that screening and referral for GD is not a part of their job.
Figure. Clinician attitudes toward screening for GD in addiction and youth service programs, with the percentage of clinicians (n = 88) who agreed/strongly agreed, felt neutral, or disagreed/strongly disagreed with each statement.
Most clinicians agreed that if a client disclosed a gaming problem they would administer a screen, conduct further assessment, or help address immediate gaming-related harms. About one-third of clinicians indicated they often or always refer the client to another agency. Clinicians reported they generally felt confident in delivering behavioral change techniques, including motivational interviewing, relapse prevention, problem-solving, and skill-building. They felt less confident in using behavioral change techniques that require gaming-specific knowledge, such as exposure therapy, social comparison, and imaginal desensitization. Finally, 58% of clinicians had attended a general information session about GD, yet few reported receiving training on screening or treatment for GD.
Why do these findings matter?
This study found that clinicians in addiction and youth service settings were largely supportive of providing SBIRT for gaming-related problems, but that challenges and barriers exist. Challenges, including lack of awareness of appropriate screening tools and low-to-moderate confidence in applying treatment techniques that require gaming-specific knowledge, might be addressed through training. Clinicians might benefit from increased education around gaming, such as the 15-hour Foundations in Gaming Disorder course. The low referral rate to external treatment or support potentially reflects the absence of referral pathways and specialized gaming treatment options in New Zealand. This finding points to the need for a comprehensive healthcare approach to support individuals with gaming-related problems.
Every study has limitations. What are the limitations of this study?
The actual prevalence of gaming-related problems in addiction and youth services cannot be determined from this study because this study only included clinicians who had provided care to at least one individual with an internet-enabled addiction. Findings from this study might not be generalizable to other types of clinical settings (e.g., primary care) and geographic locations outside of New Zealand.
For more information:
Do you think you or someone you know has a problem with gaming? Visit this webpage hosted by the Evergreen Council on Problem Gambling for treatment and support services for gaming disorder and internet addiction.
— Kira Landauer, MPH
Feb 8, 2023 | ADVOCACY
MNAPG’s outreach efforts continue in full swing. Sonja Mertz, our community educator, went through training to become a certified prevention professional. This will allow for access to prevention resources and continued involvement in prevention training.
The fall season was packed with conference and training opportunities. MNAPG hosted exhibit tables at a co-occurring disorder conference, the Addiction and Faith conference, Program Sharing conference (hosted by the Minnesota Prevention Resource Center), MARRCH (Minnesota Association of Resources for Recovery and Chemical Health) conference, Minnesota Corrections Association conference in Nisswa, Evergreen Family Services conference in Bemidji, recovery seminar at Metro State University, National Alliance on Mental Illness conference, Allied Charities convention and the Association of Minnesota Counties conference.
Sonja also had the opportunity to provide presentations at the Evergreen Conference (family and youth services) and the Allied Charities Convention (charitable gambling managers). Both audiences seemed particularly interested in youth gambling and how gaming and sports betting are impacting the gambling behavior of young people.
If you’d like to have Sonja speak to a group about gambling addiction prevention, please call (612) 424-8595.
Page 24 of 35« First«...10...2223242526...30...»Last »