May 19, 2026 | RECOVERY, RESOURCES
3/16/2026
If you’ve made a decision to stop or take a break from gambling, seeing ads splashed across social media can be incredibly frustrating and triggering.
The good news is that there are plenty of ways you can limit gambling apps across social platforms.
On most social apps, if you see a gambling ad, click the three dots and click “not interested” or “report,” which will stop the algorithm showing anything similar to you.
A lot of social apps also allow you to mute words, so you can filter unwanted content:
Examples
- gambling
- bet
- betting
- casino
- sportsbook
- bookmaker
- odds
- wager
- slots
- jackpot
Facebook
Limit Ads: Navigate to Settings & Privacy > Settings > Meta Accounts Centre> Ad Preferences > Ad Topics > Special Topics, and Deselect “Gambling”.
X
Limit Ads: Go to Your Privacy Settings > Interests From X > Toggle Off ‘Sports Betting.’
Mute Words and Phrases: Settings and Privacy > Privacy and Safety > Mute and Block > Muted Words.
Instagram
Limit Ads: Navigate to Settings and Activity > Accounts Centre > Ad Preferences > Ad Topics > Special Topic > Deselect “gambling.”
Mute Words and Phrases: Settings and Activity > Hidden Words.
TikTok
Limit Ads: Navigate to Your Profile > Click the Three Lines in the Right Corner > Settings and Privacy > Ads > Manage Ad Topics > Other > Toggle ‘Real Money Gaming’ off.
Mute words and phrases: Settings and Privacy > Content preferences > Filter video keywords.
Bluesky
Unfortunately, Bluesky doesn’t have a specific way to turn off gambling ads. However, if you see a gambling ad, click the three dots and click “not interested” or “report,” which will stop the algorithm showing similar ads to you.
YouTube Limit Ads: Go to My Ad Centre > Make Sure Personalised Ads Are Turned on > Customise Ads > Sensitive, Then Toggle “Gambling” to “See Fewer.”
Snapchat
Snapchat does not provide a category-level block (e.g., gambling, alcohol, etc.). The only control available is reducing how much data is used to target ads.
Instead, if you see a gambling ad, press down to report it, and you will start to see less content like this.
- There is peer support, and support with the criminal justice system, available at GamLEARN.
- Gamblers Anonymous isn’t for everyone, but it’s available worldwide and is a free, anonymous way to talk to others suffering from gambling harm. · The Gamban Discord is another free, anonymous platform where you can get together with others to chat, play games, or just read what others have to say.
Adapted from guidance originally published by Gamban, a gambling-blocking software provider that helps people reduce access to online gambling and gambling-related content.
May 15, 2026 | RESEARCH
Read the original article on The BASIS.
By Justin Huynh, MPH
People with a gambling disorder (GD) often experience a poorer quality of life. As a result, substantial research has explored the topic of suicidal ideation and suicide death in association with GD. However, the impact GD has on overall death risk has been less examined, especially among siblings who share genetics and early-life environmental factors that may greatly affect later life outcomes including suicide risk. This week, The WAGER reviews a study by Yang-Chieh Brian Chen and colleagues that examined how gambling disorder may be associated with suicide risk in Taiwan using both matched controls and siblings as comparators.
What were the research questions?
(1) Relative to their siblings and matched controls, to what extent do people with GD have higher risk for death by suicide, accidents, and other causes in Taiwan? (2) Are people with GD at greater risk for unnatural death, including death by suicide, even after accounting for co-occurring mental health conditions?
What did the researchers do?
The researchers used 2000 to 2022 data from Taiwan’s National Health Insurance Database to identify three groups for retrospective comparison. These groups included 961 individuals diagnosed by a psychiatrist with GD, 3844 age- and sex-matched controls, and 675 siblings of people with GD who were not diagnosed with GD themselves. The researchers used Cox regression models to estimate risk for deaths from any cause, natural causes, and unnatural causes (i.e. accidents and suicides) in each group.¹ Further, the researchers explored whether effects remained after adjusting for co-occurring mental health conditions.
What did they find?
Over a mean follow-up period of about eight years, the GD group, controls, and siblings had death rates of about 6.8%, 4.4%, and 3.7%, respectively. The GD group had a 5.50-fold increased risk for unnatural death, and an 8.84-fold increased risk for suicide, compared to the control group. Additionally, they had a 0.66-fold decreased risk of natural death (see Figure). Importantly, the increased risk of unnatural death and death by suicide remained after the researchers adjusted for mental health conditions. In comparison to their siblings who were unaffected by gambling, the GD group had an 8.65-fold increased risk for unnatural death.
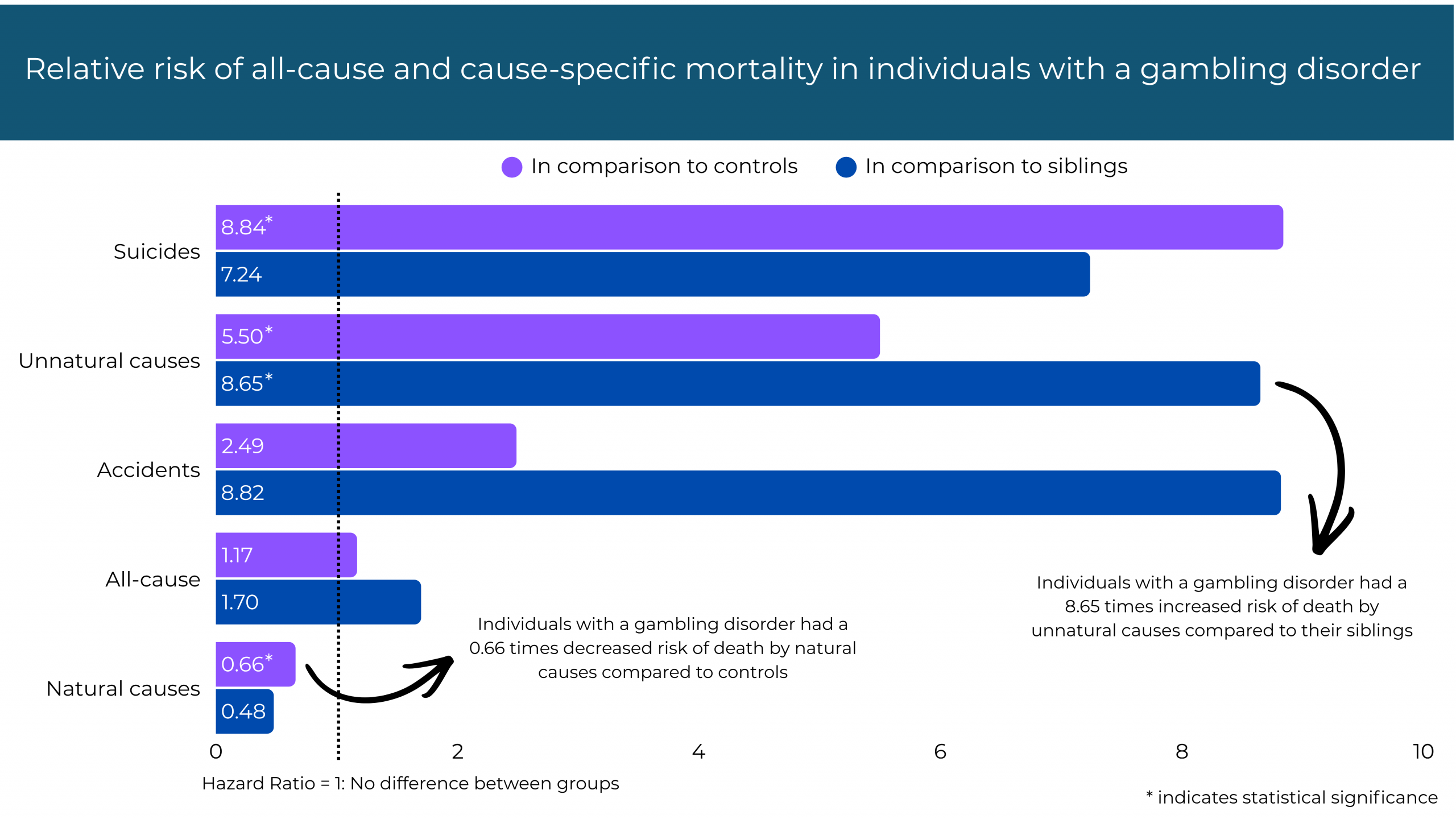
Figure. Hazard ratios for risk of all-cause and cause-specific mortality in individuals with a gambling disorder compared to controls and siblings, adjusted for relevant demographic and clinical covariates and missing data.
Why do these findings matter?
These findings emphasize that those affected by GD may be at greater risk for death by unnatural causes, especially suicide, even when accounting for other mental health problems. Those with GD or having problems with gambling should be screened for suicide risk and might benefit from education about suicidality as a potential consequence of problematic gambling. Due to the prevalence of co-occurring conditions, gambling treatment should be integrative and include screening/assessment for such conditions. Finally, gambling prevention initiatives and protections for emerging adults leaving the shared early-life environment and becoming more susceptible to gambling harms should be developed and tested.
Every study has limitations. What are the limitations in the study?
As this study was conducted on the Taiwanese population, external validity may be limited to other populations due to cultural context. While the results of the sibling comparison did result in one statistically significant finding, the small sample size of the sibling group does limit the statistical power of the analysis.
Apr 10, 2026 | PROBLEM GAMBLING, RESOURCES, SPORTS BETTING, YOUTH GAMBLING
We come across numerous articles about problem gambling and problem gaming. Here are a few:
The article reports that Washington State has sued the makers of the Bingo Blitz app, alleging it operates as illegal gambling and uses child-appealing content, weak age controls and aggressive in-app purchases that expose minors and other users to addiction risks and significant financial harm.
https://gamblingharm.org/bingo-blitz-app-illegal-gambling-children/
The column argues that the growing ubiquity and normalization of gambling—especially through sports betting and youth exposure—risks fostering addiction, financial harm and a cultural shift toward chasing quick wealth through luck rather than stable, meaningful paths.
https://www.startribune.com/brown-when-betting-is-everywhere-we-gamble-with-our-future/601567918
NPR’s A Martinez speaks with journalist and author Danny Funt about his new book, “Everybody Loses: The Tumultuous Rise of American Sports Gambling.”
https://www.npr.org/2026/01/19/nx-s1-5602138/everybody-loses-chronicles-the-rise-of-americas-sports-betting-boom
A piece by PBS on How Sports Betting is changing our Brains and Behavior, features Danny Funt and Dr. Tim Fong.
https://www.pbs.org/newshour/video/horizons/2026/02/how-sports-betting-is-changing-our-brains-and-behavior
This Teach-Out is open to anyone interested in learning more about the sports betting industry and its effects on the general population, but it is particularly relevant for young adults and their parents, athletes, educators, and policymakers looking to mitigate the effects of sports betting.
https://online.umich.edu/teach-outs/sports-betting-risks-and-ripple-effects-teach-out/
Apr 10, 2026 | ADVOCACY, RESEARCH
For the first time, federal research funding will be available to study gambling addiction. The fiscal year 2026 defense appropriations package includes language allowing gambling disorder to be researched through the Department of Defense’s Peer Reviewed Medical Research Program (PRMRP).
The Senate report clarifies that gambling addiction is an eligible research topic under the program. While the funding is limited to military and veteran populations, the change represents the first time a federal medical research program has explicitly supported peer-reviewed research on gambling addiction, reflecting growing recognition of the issue as a public health concern.
The inclusion is especially relevant for servicemembers and veterans, who face elevated risk for gambling-related harm. Research has found strong links between gambling disorder and suicide risk; among veterans seeking treatment for a gambling problem, nearly 40 percent report a suicide attempt. Military populations may also experience higher exposure to risk factors such as stress, trauma and ready access to high-risk gambling environments.
Gambling addiction has historically received little attention in federal research portfolios, leaving gaps in evidence to guide prevention, early intervention and treatment. Advocates say expanding research access is an important step toward improving understanding and care for affected populations.
This funding must be appropriated each year. NCPG will be closely monitoring and working with their lobbyists to support funding renewal.
Apr 10, 2026 | RECOVERY, SPORTS BETTING, YOUTH GAMBLING
When I quit using alcohol and drugs, I thought that was the hard part. What I didn’t realize was that I had created a huge void in my life. I wasn’t getting those instant dopamine hits anymore, and I didn’t know what to do with myself. That’s when gambling quietly slipped in.
My gambling didn’t start in a casino or with sports betting like it does with a lot of people. It started, oddly enough, with clothes.
When I was in college, streetwear was big. There were online raffles for limited-edition clothing. You’d throw in $10 or $25 for a chance to win something worth a lot more. I started doing those raffles all the time. If I won, I’d try to resell the item. Before long, I was doing this every single day—including watching the raffle videos—while having basically no money. That should’ve been a red flag, but I didn’t see it that way at the time.
I did the clothing raffles for about two years and then stopped gambling for about a year. Then I started playing fantasy football with friends and things gradually progressed. I started doing future bets, like whether a team would win the championship or how it would do for the whole season. Then it became point spreads and over/unders for individual games. Then it became in-game live betting. That all felt “manageable,” at least compared to what came next.
My sports betting got worse. DraftKings wasn’t what it is today, so I used an illegal offshore site. It started small with $5 and $10 bets, but gradually turned into betting every day, multiple times a day. I was betting on games I didn’t even watch or know anything about, like baseball games in a league on the other side of the world. That made it harder to lie to myself that this was just for fun.
What really pushed me over the edge was online casino gambling. While watching sports, I started clicking into online casinos on my phone for fun. I quickly went through five-dollar slots and started chasing my losses. Then I’d lose $100 trying to get it back on roulette or blackjack. I started using money I didn’t have—dipping into credit cards and debit cards. I wasn’t paying rent and was barely eating. I had a decent job and still couldn’t afford to live.
I was living with my girlfriend at the time, as gambling slowly took over my life. I’d get home from work and watch games from 4 p.m. until midnight instead of spending time with her. She had no idea how bad it was. When she eventually broke up with me and moved out—taking the dog—I couldn’t afford the apartment on my own because of gambling.
I had only been to one or two GA meetings at that point, so I didn’t really have a GA program. I asked someone in AA if they knew anyone who had been to GA, and I got connected with someone who offered to take me to a meeting. He became my GA sponsor. I thought it would be just like AA—and at a high level it is—but it’s clearly different because I couldn’t manage my gambling addiction as well as I managed my alcohol addiction.
I was surprised how few young people were in the GA rooms. Given how much I know younger people are gambling, particularly on sports, I’d expected more people in their 20s and 30s. I found that many of the people went to live casinos and played a lot of scratch-offs, activities I think are less common in my age group.
As I look back on my gambling, I wasn’t really chasing wins; I was chasing a feeling. I don’t even remember having many big wins. No win ever felt that good and every loss felt awful. I just wanted to feel something, or avoid being present in my own life.
After I stopped gambling almost two years ago, I couldn’t watch sports for a long time. I’d always think, “I would’ve won that if I’d bet.” Eventually, I was able to watch again, but the ads are everywhere now. I honestly can’t imagine trying to quit for the first time today with all those reminders.
I just turned 30. I still get urges to gamble more than I ever get urges to drink. Gambling ads hit me in a way alcohol ads don’t. I also see how normalized betting has become, especially for younger people. My little brother is in college, and betting is just part of the culture—everyone seems to be doing it. I try to keep the door open so he knows he can talk to me if it ever becomes a problem.
Thankfully, life today is much more manageable. I know my brain is always going to look for something, so I try to channel that energy into healthier things—running, relationships, being present. I’m not perfect, but I’m honest now. And that makes all the difference.
If any of this sounds familiar, I promise you’re not alone—and that there is hope. Help is out there. Recovery doesn’t make life perfect, but it does make it livable—and for me, that’s more than enough.
Page 1 of 3712345...102030...»Last »