The term “addiction” is defined as the state of being compulsively committed to a habit or practice or to something that is psychologically or physically habit-forming, such as narcotics, to such an extent that its cessation causes severe trauma.
Most of us are familiar with certain addictions, even if we may not completely understand them. For example, many of us know the person who can’t stop drinking, the person who can’t stop using prescription medications or the person who can’t stop using illicit drugs.
Yet there are many other addictions, ranging from food addiction to sex addiction to video game addiction. One addiction that’s as real as any but which is under reported in the media, and under recognized and under diagnosed by the treatment community and the general public, is gambling addiction.
This article will show how gambling addiction is essentially similar to other addictions and, indeed, merits the funding, attention and treatment that other, more commonly known, addictions do.
The Addicted Brain
While the range of addictions might seem different on the surface, there are certain fundamental things that they have in common. In particular, the processes that take place in the brain of a person with an addiction are quite similar.
When a person gambles for the first time, they might find it exciting. They might win money and feel on top of their world. This experience registers in their “reward hub” (ventral striatum), which acts like a gas pedal in their car to get them to where they want to go. The “control network” (pre-frontal cortex) works to stop or slow down what they’re doing. When these two areas are working together, the person is in control of their behavior and knows when to stop.
Addiction takes place when these two areas of the brain are not communicating properly. Continuing with the car analogy, an addict keeps pressing on the gas only to learn that the brakes may not work. By the time someone realizes they may have a problem with their gambling, it can be difficult to stop because it’s become a habit. Habits are developed when the brain no longer exercises conscious control. The person is essentially on autopilot. They become very aware of gambling cues and triggers, such as sporting events or casino or lottery advertisements.
At this point, gambling isn’t as fun as it was in the beginning. However, the addicted gambler continues gambling to escape the uncomfortable urges that the triggers create with the hope of recreating the high that they experienced early on in their gambling activities.
As the consequences of one’s gambling get worse, so does their mood. Whereas gambling once had a positive effect on their mood, it now cycles downward. Over time, they find gambling less pleasurable, and their mood continues to get worse, even when no longer gambling.
SEE ALSOFrom MN DHS: As Sports Betting Goes Mainstream, So Must Problem Gambling Awareness
The brain processes that take place in people with addiction have been borne out by recent studies. Analyses of brain imaging of people with substance addictions and people with gambling problems show that both have less activity in the reward hub than people without addictions when it comes to anticipating rewards.
Over time, they find gambling less pleasurable, and their mood continues to get worse, even when no longer gamblingA person with an addictive brain is operating from the deep limbic brain (the place where emotion and survival are housed) and bypassing the frontal cortex (where logic and reason reside). People with addiction don’t choose for their brains to respond in this way, it’s the demand for dopamine that forges these distorted messages and strengthens these unhealthy pathways in the brain. An addicted brain is literally sending the message of survival when it is seeking another infusion of dopamine.
This means that people with addictions don’t process rewards in the same way. They may not be as excited by natural rewards. They might also have trouble learning how new experiences, such as taking up a hobby for the first time, can be enjoyable. That is why some people might seek out unnatural rewards (like gambling, alcohol, or drugs) just to feel pleasure or to escape.
Addictions hijack the attachment system, meaning that when a person is addicted to something, they gradually grow more detached from their personal relationships and responsibilities. They lose their true selves. Philips Flores, PhD., describes addiction as “a disease of isolation.” As the disease progresses, the gambler prefers to be alone, not wanting anyone to disrupt their “flow,” even if they are in the midst of chasing losses.
The good news is that brains are continually changing. Therefore, the processes that create addiction can be reversed to a varying degree over time. A study published in Neuropsychopharmacology showed that the brains of individuals with substance-based addictions changed in response to non-addiction cues. This means that individuals recovering from an addiction can start to enjoy natural rewards again. However, because these changes can take time to occur, it emphasizes the importance of continuing to practice previously enjoyable hobbies, to try out new activities in new settings, and to be around those who engage in positive behaviors. For those who choose recovery, it’s a journey that includes breaking from addictive habits and learning to reconnect to people and activities that will promote wellbeing, satisfaction, and joy.
Given the time it takes to build new brain processes—and a lasting recovery—individuals should consider the importance of cultivating healthy responses to non-gambling rewards. This can help protect them from the dangers of cross addiction and relapse, and create a rich, meaningful, and rewarding life over the long term.
Similar, But Not Equal
Given the similar processes involved with all addictions, it’s not surprising that some individuals “switch” from one type of addiction to another (also known as substitution or cross-addiction). For example, when a person stops drinking, he may find himself smoking more cigarettes, binging on certain foods, or gambling excessively. This unfortunate occurrence can occur because of reduced activity in the reward hub and their ability to “brake,” making a person vulnerable to other unhealthy rewards to satisfy urges. The result could be a new pattern of repeated rewarding behavior that steals one’s attention, opening the door to a new addiction.
With recent technological advancements, brain scans clearly show the commonalities of substance addiction and gambling addiction. In fact, it was in 2013 when the DSM-V (Diagnostic and Statistical Manual for Mental Health Disorders) finally recognized gambling as a peer addiction to substance addiction.
Given the similarity of the underlying process involved with all addictions, it’s logical and necessary for gambling addiction to be viewed through the same lens as substance use addiction. Fundamentally there should be appropriate and commensurate support in the form of funding. Unfortunately, funding for gambling treatment and prevention is a mere pittance of monies spent on treatment and prevention of alcohol and substance abuse.
In the U.S., substance use disorders are about seven times more common than gambling disorders, yet public funding for substance use treatment is about 338 times greater than public funding for problem gambling services. There are no federal funds for gambling disorder; all funds are provided by the states.
In Minnesota, there are no prevention materials on gambling addiction in the schools. While services offered to those seeking substance use treatment include opportunities to meet with certified peer recovery specialists, no such service is provided for problem gamblers. Minnesota has county-operated behavioral health clinics, yet they don’t offer services for problem gambling, nor is any screening for gambling addiction available. These clinics receive most of their funding from the federal government and adhere to federal regulations. While these clinics promote themselves as one-stop shops for all mental health and substance addictions, they do a significant disservice to those who may have gambling co-addictions by not screening for this disorder.
Reforms are needed for Minnesota’s approach to gambling addiction. Part of the mission of the Minnesota Alliance on Problem Gambling (MNAPG) is to advocate for parity of services and increased funding, along with educating the general public and treatment community that gambling addiction is very real.
An Equal Opportunity Addiction
Gambling addiction doesn’t discriminate by race, gender, socioeconomic status, culture, or age. Treatment for this often-devastating addiction is available — and it works. If you know of someone in your life who may be exhibiting signs of gambling addiction, let them know that help is available at no cost. Referrals are available through the Minnesota Problem Gambling Helpline at 1-800-333-HOPE (4673). MNAPG’s website has a wealth of information and resources on gambling addiction.
When kids turned eighteen in Minnesota, a favorite way to highlight the occasion, especially in the early 2000’s, was with a night out at a nearby casino. They celebrated their milestone birthdays with all the exuberance of youth who’ve reached the legal age to participate in an adult activity. Most adults continue to enjoy occasional nights out at a casino. They gamble from time-to-time without any serious consequences to their health, relationships, and finances. Not everyone is as lucky.
Consider Barbara* (The name Barbara is being used to protect her anonymity), a recovering compulsive gambler, who shared her story with The Phoenix Spirit. While on her honeymoon in the Bahamas, she played low stakes games, had fun, and viewed it as simple entertainment. When she got home, she gambled once, and didn’t enjoy it. For a few years, she didn’t gamble at all. However, in 1995, when she moved to a small town, started a business, and came under a lot of stress, she viewed the casino as a place to get away from it all, to think, relax, and have fun. When her husband lost his job and the financial pressures increased, casinos became more than just entertainment. She went with the idea, “Let’s see if I can win some money to pay the bills.”
On my first attempt, I hit the jackpot, the endorphins kicked in, and I was hooked.For the next six years she went off-and-on, sometimes stopping completely if she’d had a bad episode and lost a lot of money. As a couple, she and her husband identified gambling as a problem. In 2001, they wanted to have another baby and went to the Mayo Clinic for fertility treatment. During one of the pre-treatment screenings, her husband brought up gambling as a concern. The screening team said, “We won’t do the fertility treatments until you deal with the gambling. We’re referring you to a treatment center in Granite Falls.”
Barbara said, “I thought they were crazy. I believed I could stop on my own. I did stop for 18 months. We went back to the Mayo Clinic, and we successfully proceeded with the treatment. However, I had a miscarriage, and after that, I had a really rough time. I just wanted to escape from the world, escape from my problems, and I sought comfort and peace through gambling.” Her use escalated, she and her husband started having marital issues, and they separated in 2006.
One of her business clients told her about his high stakes gambling. She decided, “I’m giving that a try. On my first attempt, I hit the jackpot, the endorphins kicked in, and I was hooked. I moved from blackjack betting to slot machines to high stakes slot machines.”
In her loneliness, Barbara’s use escalated for the next four years, until she said, “Man, this is hurting me a lot. I’m going to stop at the end of 2009.” She did stop. She wasn’t in a formal program; she wasn’t familiar with any 12 Step program. She reconciled with her husband in 2010.
In 2011, something set her off, and she went right back to the casino. For the next six years, she gambled off-and-on quite a bit. She lost substantial amounts of money. She still paid her bills, but wasn’t saving the way she should have, juggled accounts, and robbed from the proverbial Peter to pay Paul. She thought she was only hurting herself, that her gambling wasn’t causing any big family problems, but she’d go to the casino at night, and not be in any shape in the mornings to get her daughter to school. Her marriage was on the rocks again. Her husband lost his job. They eventually divorced.
In 2016 she tried everything she knew to stop. She banned herself from casinos and canceled all her accounts. Yet she couldn’t stop. She’d go back to the casinos, thinking, “If I just don’t carry credit cards or cash cards with me, I’ll be okay. But as everybody knows, the casinos still had a way to get my money.”
Finally, in 2017, Barbara had had enough. She took a month off from her business, and went through treatment at Project Turnabout/Vanguard, Minnesota’s one treatment center focused only on gambling addiction, what Barbara calls ‘an eye-opening experience.’ Counseling sessions helped her recognize the unresolved grief from a traumatic event in her early twenties. Yet, when she got out, she thought it would be easy; that she wouldn’t have to work the program.
“I thought I could just quit on willpower. At 90 days, when I should have been at a Gambler’s Anonymous (GA) meeting getting a keychain {given to members at 30/60/90 days, 6 and 9 months}, I went gambling with a couple of other friends. I spiraled down into a lot of hell. I just gambled pretty hard. I’d have 5 months of not gambling and then relapse, 2 months and then relapse.”
In 2019, a cruise line offered her a free trip with free play. She went with a friend with the intention that her friend would get the free play. “I was in casino jail for a week. I hit rock bottom. I started all the gambling behaviors all over again. The juices got going, the dopamine hits took over. For the entire week, I hardly slept, maybe an hour-and-a-half at night. When I got off the ship, I looked terrible. I’d spent enough in a week to buy a new car.”
Barbara knew something had to change. “I started going to GA meetings regularly. I got a sponsor. Two meetings a week are what it seems I need to stay focused on my recovery. Even though I don’t drink much, Friday nights are when I like to ‘party.’ Now, I’ll go to a recovery meeting on Friday nights to get me through the weekend and a Tuesday meeting. I started other recovery strategies, too. I’ve been a panelist at a mini-conference on gambling and I volunteer to speak at Vanguard, the gambling unit of Project Turnabout.”
When asked about going in and out of recovery, Barbara said, “I would say I was “abstinent” from gambling more than in recovery. True recovery is different than abstaining. It’s a way of life. It’s a way of thinking. When you abstain, you’re still vulnerable. When you’re actively working a recovery program, actually working the 12 steps, and understanding what they mean, it’s different. People have a lot of amends to make. As an addict you have a lot of behaviors, you lie, you cheat, you steal.”
“For me, in recovery, I’m trying to make amends. My gambling was very hurtful to both my ex-husband and my daughter. She’s grown now, but my gambling affected our relationship quite a lot. My daughter felt that it created a coldness between us. I thought I’d always provided for her. I helped her pay for college, buy a car, and supported her. I went to all these activities. However, I was shocked at what she said in the family program. She felt that I was distracted and not really present with her. Making amends is a big part of a recovery program and can take a lifetime. That’s way different than stopping gambling and abstaining. Making amends doesn’t happen overnight.”
When Barbara got serious, in May, 2019, she made it through the first 90 days and kept going. In March 2020, all the casinos closed due to Covid. For her, that was a really good thing. “Covid was a challenging time for my business. I had a lot of issues with employees being gone, out sick, and out due to quarantine. I’m in the financial industry and it was a tough business for a couple of months with so much uncertainty. It was rugged. During Covid, nobody wanted to meet in person and we couldn’t meet anyway because churches were shut down. Project Turnabout started an online recovery meeting that met every Tuesday night up until last summer. I went to that meeting and then every Friday night I dialed in to a phone meeting. That was my trek from starting recovery to celebrating recovery.”
Marti Paulson, the CEO of Project Turnabout/Vanguard, described the center where Barbara went for treatment. “Our center has 20 residential beds for men and women. We treat co-occurring disorders, and hire mental health practitioners to work with the gambling addiction counselors. We hire registered and licensed nurses and counselors. Patients are given very individualized treatment plans. The 30-day stay also includes a one-day program where families can come or they can participate via Zoom. Gambling is a family disease and affects everyone, the same as any other addiction. To leave the family untreated would be a severe injustice.”
“We at Project Turnabout take a neutral stance to gambling. One of the reasons we do is that alcohol and gambling are legal in Minnesota. We want to be there when individuals and families are ready to get help. Second, we receive grants and a great amount of support from the casinos and resorts, both in Minnesota and from other states. We don’t want them to think that we’re against them.”
“Minnesota is a little different from other states. The State of Minnesota will pay for any state resident or family member to go for residential gambling treatment. There isn’t another state in the United States that does that. The funds are obtained through the unclaimed lottery fund, as well as from .05% of the stadium fund. Unlike chemical dependency treatment which is covered through Medicaid and state covered PMAP insurance, gambling treatment is not. It’s a little-known fact that Minnesota offers free treatment for those seeking help for problem gambling.”
When asked about the trends in problem gambling, Ms. Paulson noted that there has been an increase. “We saw the after-effects of Covid take quite a toll on gamblers. Covid shut down casinos. Going to casinos became difficult. Instead, online gambling increased – pool shooting gambling, card playing, sports betting – much more so than the typical casino gambling. Gamblers are very strong isolators.”
In 2018, the Supreme Court overturned a nationwide ban on sports betting. Since then, nearly three dozen states have passed legislation approving sports betting. On Feb. 20, 2023 companion bills were introduced in the Minnesota House and Senate that would legalize retail and online sports betting in the state. The tribes would have exclusivity with sports betting. {As we go to print, no votes have been taken.}
According to Ms. Paulson, in the past, many more men than women struggled with problem gambling, however in the last ten years, similar to alcoholism, the statistics have equaled out to almost 50/50. It’s become much more acceptable for women to go into both bars and casinos. “We’re seeing lots more young people with gambling addiction. Youth are much more likely to be involved in online gambling. We don’t take anyone under the age of 18 in our residential treatment program. The only residential treatment facilities for young people are out state. Gaming is a whole industry within itself. Although gaming addiction is treated much the same as gambling, gaming has a much different, younger population.”
When asked how sports betting factors into these trends, Susan Sheridan Tucker, Executive Director of the Minnesota Alliance for Problem Gambling (MN APG) stated, “Sports betting is primarily done by young men, ages 18-30. The sports gaming operators are trying to lure more women into gaming by changing the look of games so that they’ll appeal to women. Lots of women enjoy sports. The operators are hoping women will also enjoy sports betting. They’re using the terms ‘sports betting’ and ‘gaming’ to smooth over the negative association people have with ‘gambling.’ The mobility, accessibility, and lure of online gambling is concerning. Igaming – which is essentially any casino-type game that is also electronic – can be free to start. These games mimic slot machines, poker, and standard casino games. They allow you to play for free for a fixed amount of time or for so many wins. If you want to continue to play, you need to pay. The gaming operators know how to hook people.”
Minnesotans are very fortunate to have the longest-running residential treatment center in the US and to have their treatment paid for through state funds. When asked if people are taking advantage of this opportunity, Ms. Sheridan-Tucker replied, “Not as many as they should. Right now, only 100 people are in treatment. Research shows that 0.05 – 2 percent of the population has a severe gambling problem. That’s 250,000 Minnesotans, and 10,000 high school students. Nationally, 400 times more is set aside for substance use addiction than for gambling addiction. Yet the brain acts the same way with both.”
Funding for prevention, research and treatment and increased awareness by the public of the issues surrounding problem gambling, online gaming, and sports betting could help so that the next group of high school seniors who go out to celebrate their 18th birthdays will be able to avoid the pitfalls of compulsive gambling. There is hope, there is recovery.
The Minnesota Alliance on Problem Gambling is raising awareness about gambling addiction, as it predicts nearly $10 billion in both legal and illegal bets to be placed during this year’s NCAA Men’s Basketball March Madness.
According to a new survey by the American Gaming Association, 68 million American adults plan to bet on the tournament, meanwhile, 4 – 6 million of which are considered to have mild or moderate gambling problems.
Warning signs of problem gambling include betting more than you can afford to lose, bragging about your wins but never the losses, lying about the amount you’re betting, and spending long periods of time gambling or betting more frequently.
With a majority of people making brackets and bets online, it’s easier to develop these harmful habits.
“The electronic accessibility makes it easier, it also makes it easier for someone to isolate. You can now sit in your home on your phone and nobody knows,” says MNAPG Executive Director Susan Sheridan Tucker. “It’s not that we’re against gambling, we just want it to be safe for all players.”
Some precautions to take when it comes to gambling include setting a time limit, setting a spending limit, checking in with how you feel, and being honest with yourself.
Problem Gambling Awareness Month is also about raising awareness about for resources available to those who do need help with problem gambling.
“There’s a variety of ways that people can approach recovery. For some, it means total abstinence, that’s the way in which it’s going to be helpful for them. For others, it may be just adjusting, that they pull back, take a break,” says Tucker.
Editor’s Note: Today’s review is part of our month-long Special Series on Pathways to Addiction. Throughout March, The BASIS is highlighting risk factors for and pathways to addiction.
The development of the pathways model of problem and pathological gambling in 2002 was an important step towards recognizing the heterogeneity of individuals who face gambling-related harms. The model identified distinct subgroups of people experiencing problem or pathological gambling based on a variety of social, biological, and environmental risk factors. The authors, Alex Blaszczynski and Lia Nower, identified three distinct subtypes of individuals experiencing gambling problems: (1) those who were behaviorally conditioned, (2) those with pre-existing emotional vulnerabilities (e.g., anxiety, depression), and (3) those who reported frequent impulsive and/or antisocial behavior. This week, as a part of our Special Series on Pathways to Addiction, The WAGER reviews a study by Lia Nower and colleagues that updated and revised the original pathways model.
What were the research questions?
Does the pathways model of problem and pathological gambling require revision? What revisions or additions should be made to the pathways model?
What did the researchers do?
The researchers surveyed 1,168 individuals with moderate to severe gambling problems seeking treatment across the United States, Canada, and Australia. Participants completed the Problem Gambling Severity Index (PGSI) and the Gambling Pathways Questionnaire (GPQ). The PGSI is a well-regarded and frequently used research instrument to measure the presence and severity of an individual’s gambling problems. On the other hand, the GPQ is an instrument designed to categorize individuals experiencing problem gambling based on the risk factors that they might have experienced. Using participants’ scores on the 11 subscales of the GPQ, the researchers performed latent class analysis to identify subgroups of individuals experiencing problem gambling.
What did they find?
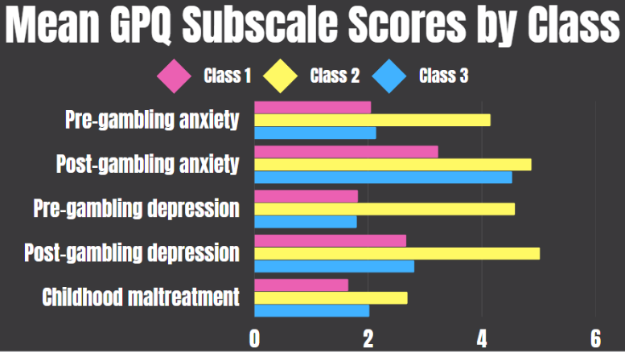
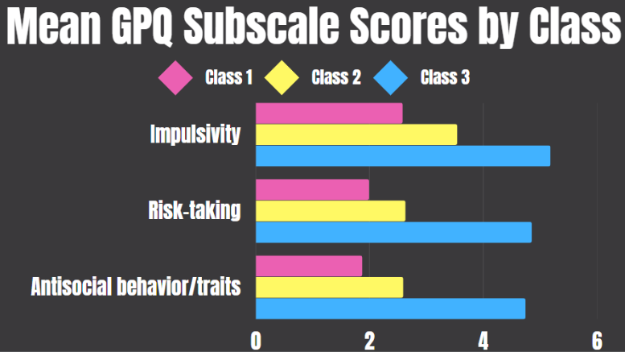
Similar to the original pathways study, the latent class analysis identified three distinct subgroups. Class 1, the largest class, had the lowest average (i.e., mean) scores on each of the GPQ subscales. Class 2 was characterized by high levels of anxiety and depression, both pre- and post-problem gambling, in addition to a high rate of childhood maltreatment (see Figure 1). Finally, Class 3 comprised individuals who scored high in impulsivity and reported frequent risk-taking and/or antisocial behavior (see Figure 2). In terms of problem gambling severity, Class 2 had the highest average scores, while Class 3 scored only slightly lower. Notably, the research team also found some overlap between classes. For example, Classes 2 and 3 both reported gambling to cope with stress, though only Class 3 reported gambling to find meaning.
Figure 1. Gambling Pathways Questionnaire (GPQ) subscales that differentiate Class 2 from Classes 1 and 3. The total possible range for each GPQ subscale varies and is calculated by summing the responses within each subscale. Click image to enlarge.
Figure 2. Gambling Pathways Questionnaire (GPQ) subscales that differentiate Class 3 from Classes 1 and 2. The total possible range for each GPQ subscale varies and is calculated by summing the responses within each subscale. Click image to enlarge.
Why do these findings matter?
Recognizing the heterogeneity of pathways to problem gambling within this population is important because it allows treatment professionals to focus on the most salient risk factors for gambling problems rather than more tangential issues. For example, impulsivity is considered an important risk factor for Gambling Disorder and some interventions focus on modulating impulsivity. However, because only a subset of participants experienced heightened impulsivity, it is possible that significantly more people who experience gambling problems would instead benefit from safer product design that disrupts the conditioning aspects of gambling, such as mandatory breaks or the use of self-limit features (e.g., limiting time or amount wagered per gambling session).
Every study has limitations. What are the limitations in this study?
This study only included individuals who were seeking treatment for Gambling Disorder, so the findings might not apply to non-treatment seeking individuals experiencing gambling problems. Additionally, the GPQ measures pre-gambling anxiety/depression by asking participants to retrospectively recall their feelings though research suggests these measures are unreliable.
Legislation needs to include increases in treatment, prevention and research funding to match the proposed expansion of gambling rights.
By Susan Sheridan Tucker
Opinion editor’s note: Star Tribune Opinion publishes a mix of national and local commentaries online and in print each day. To contribute, click here.
•••
March Madness is well underway, and with it a deluge of gambling that propels the tournament. It’s estimated that 1 in 5 Americans will place bets on this year’s NCAA basketball tournament, which creates a hazardous environment for anyone susceptible to problem gambling.
Though most Americans can gamble for enjoyment without issue, the issue of gambling addiction is one that’s gone woefully unaddressed by state and federal addiction programs. It is a fact that gambling addiction produces the highest rate of suicide among addictions, making it a very real public health issue.
As Minnesota lawmakers consider passing a bill that would legalize sports betting, it’s more imperative than ever that the legislation includes increases in treatment, prevention and research funding to match the proposed expansion of gambling rights. It is the mission of the Minnesota Alliance on Problem Gambling (MNAPG) to raise awareness of gambling addiction and advocate for more safeguards around gambling to ensure consumers are protected and able to access resources for treatment and prevention.
It’s no coincidence that March is Problem Gambling Awareness Month. All over the country, organizations like ours make special efforts throughout the month to get the word out that problem gambling is a legitimate addiction defined in the latest edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
Though MNAPG remains neutral on legalization, we stand for the prioritization of consumer protection over revenue. We’ve worked alongside several lawmakers involved in crafting the proposed legislation, which includes a lot of promising language around the following:
Funding: Directing 40% of sports betting tax revenue toward problem gambling programs.
Age restrictions: The promise to raise the legal betting age to 21 will help to prevent high school students from accessing regulated gambling sites on their phones.
Education: Prevention messaging to students, and especially young athletes, will provide a foundational understanding of the harms that can occur with gambling and where one can turn for help. Gambling prevention education is still absent from middle school and high school curricula.
Meanwhile, there are key pieces missing from the current legislation that would be critical to include. They include:
Rule making: MNAPG would prefer to see more specific language built into the bill and will actively participate in the rule-making process to include specific practices requiring operators to build responsible gaming programs. These programs should include comprehensive employee training, access to self-exclusion programs, ability to set limits on time and money spent on betting, and specific requirements for the inclusion of help/prevention messages in external marketing.
Research: There are currently no federal dollars to fund gambling disorder research. Each state must decide whether to support such efforts. MNAPG believes there should be funding for regularly scheduled studies to monitor the impacts of gambling on players and support for using the data to develop evidence-based mitigation efforts. We don’t seek individual data, but would make aggregate data on players’ behaviors and experiences available to universities and nonprofit research entities. Without access to such data, the hands of those who work in the prevention and treatment fields are tied.
No one chooses to become addicted to anything — it’s never due to a moral failing or a lack of willpower. Gambling addiction is just as serious as an alcohol or drug addiction and deserves to be treated equitably, with an appropriate level of funding for treatment, prevention, research and training.
Susan Sheridan Tucker is the executive director of the Minnesota Alliance on Problem Gambling.